Preeclampsia, a pregnancy-linked blood pressure disorder, affects 3-4 percent of pregnancies in the United States, or approximately 177,000 women as of 2014 (a 21 percent increase since 2005!). Here’s everything you need to know about the signs and symptoms, risk factors, and complications, as well as treatments and prevention.
What is preeclampsia?
Preeclampsia is a pregnancy complication that develops after 20 weeks and involves hypertension (high blood pressure) and minor to severe organ damage in a woman whose blood pressure was previously normal. It is one of the leading causes of maternal death in the United States. And more rarely, preeclampsia can develop up to six weeks postpartum (more on that in a bit). You might have also heard preeclampsia referred to as toxemia, pregnancy-induced hypertension, or preeclamptic toxemia. It’s also possible to develop hypertension during pregnancy without developing preeclampsia—this is usually called gestational or transient hypertension.
So while symptoms can often be managed, ultimately the only “cure” for the condition is to deliver the baby and placenta.
Preeclampsia is caused by abnormalities in the placenta, the organ that provides your baby with oxygen, nourishment, and waste management during pregnancy. Unfortunately, it’s not clear what causes these abnormalities, which include lesions or issues where blood vessels don’t develop normally. It takes a lot of blood vessels to facilitate the exchange of oxygen, nutrients, and waste between mothers, placentas, and fetuses, so when this happens, the placenta doesn’t receive enough blood. These issues can occur very early in pregnancy, but there are no good tests to determine who will develop preeclampsia. So while symptoms can often be managed, ultimately the only “cure” for the condition is to deliver the baby and placenta.
Who’s at risk for preeclampsia?
Any pregnant woman can develop preeclampsia, but certain factors can raise your risk:
- First pregnancy
- History of preeclampsia (personal or immediate family)
- Chronic hypertension, kidney disease, lupus, migraines, diabetes, or other chronic illnesses prior to pregnancy
- New paternity
- Age (younger than 20 or older than 35–40)
- Carrying multiples (twins, triplets, etc.)
- Race (black women are at higher risk)
- Obesity
- Pregnancy interval (less than 2 or more than 10 years apart)
- In vitro fertilization (IVF)
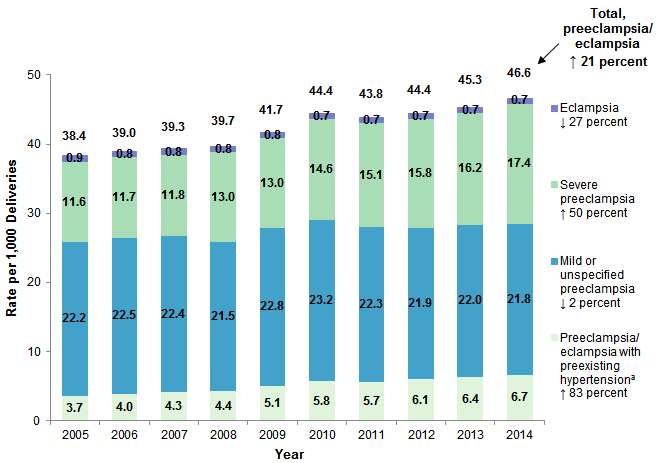
And though it’s unclear why, preeclampsia has been on the rise.
Source: HCUP Statistical Brief #22, Delivery Hospitalizations Involving Preeclampsia and Eclampsia, 2005-2014
What are the signs and symptoms of preeclampsia?
Many women with preeclampsia never experience any reportable symptoms, so keeping your regular prenatal visits is key; screening for preeclampsia is part of why you find yourself going to so many more appointments when you hit the third trimester. Some of the warning signs of preeclampsia (like nausea and vomiting or swelling) happen frequently during healthy pregnancies as well—but you should always keep an eye out and make sure you report any concerning signs or symptoms to your healthcare provider ASAP.
Many women with preeclampsia never experience any reportable symptoms, so keeping your regular prenatal visits is key; screening for preeclampsia is part of why you find yourself going to so many more appointments when you hit the third trimester.
These are some of the most common signs and symptoms of preeclampsia:
- New-onset hypertension (140/90, on at least two occasions, at least four hours apart)
- Proteinuria (excess protein in your urine; a small amount—under 150 mg/day—is considered normal, but double that is a red flag)
- Severe headache
- Upper abdominal pain (often on right side)
- Nausea and vomiting
- Sudden shortness of breath
- Vision changes (like blurred vision, blind spots, flashes of light, or loss of vision)
- Decreased urine output
- Low platelets (platelets help your body form clots to stop bleeding)
- Impaired liver function
- Sudden weight gain
- Sudden swelling, especially in hands and face
What are the complications of preeclampsia?
High blood pressure is one of the most obvious signs of preeclampsia, but it has far-reaching effects. Because preeclampsia arises from abnormalities in the placenta, which is nourishing the baby, many of the complications involve the baby’s growth, maternal and fetal blood vessels, and the placenta itself. Preeclampsia does not get better on its own—and if left untreated can get much worse (and even be deadly). Interventions are often necessary for the health and safety of both mother and baby. Most cases of preeclampsia develop after 37 weeks, and in these cases, delivery is often the best option.
These are some of the most common complications of preeclampsia:
- Fetal growth restriction (when baby’s growth slows due to reduced blood flow and nutrients from the placenta)
- Preterm birth
- Maternal organ damage (kidneys, liver, lungs, heart, eyes)
- Eclampsia (preeclampsia plus seizures)
- HELLP syndrome (severe form of preeclampsia that can quickly become life-threatening)
- Placental abruption (when the placenta separates from the uterus before delivery; in severe cases it can cause life-threatening bleeding)
- Stroke/brain injury
- Cardiovascular disease (having preeclampsia can increase your future risk of heart and blood vessel disease)
Admittedly, this list is pretty terrifying, but the good news is that most cases of preeclampsia occur close to full term (reducing the risk of preterm delivery), and with regular prenatal care preeclampsia can often be identified early. It’s also important to keep in mind that not everyone who develops preeclampsia will experience these complications, but they are good to be aware of.
What to expect if you are diagnosed with preeclampsia
The bottom line is that treating preeclampsia means balancing the health of the mother and the baby, because while delivering the placenta usually addresses things for the mother, that isn’t a viable option for many preterm babies. Everyone’s situation is different, and your providers will take all kinds of factors into account when determining next steps, including how far along you are, the severity of your preeclampsia, and any complications you’re experiencing.
Because preeclampsia arises from abnormalities in the placenta, which is nourishing the baby, many of the complications involve the baby’s growth, maternal and fetal blood vessels, and the placenta itself.
You’ll likely have some blood work done and may also be asked to complete a 24-hour urine collection, so your provider can get an accurate picture of how much protein is in your urine. If your preeclampsia is mild—that is, you’re showing some symptoms that don’t need immediate intervention, like high blood pressure that isn’t so high you’re at risk for a stroke—it’s possible your providers may continue to monitor you and the baby closely (either in the hospital or with more frequent check-ups) while delaying delivery. Common measures in this case include complete or partial bed rest, antihypertensive therapy to prolong pregnancy, and corticosteroids for fetal lung maturity.
If your provider decides delivery is the best option, your labor may be induced with Pitocin, a medication used to start labor, and a synthetic version of the hormone oxytocin, which our bodies produce naturally. In many cases of preeclampsia, a vaginal delivery is still possible, though an estimated 53.9 percent of cases end in C-section.
Keeping follow-up appointments after your baby is born is key.
If your blood pressure skyrockets either before or during labor, you’ll likely be treated with medication to bring it down into a normal range to prevent stroke and damage to your blood vessels. Because it’s very hard to determine who will develop seizures, women diagnosed with preeclampsia are often treated with magnesium (which is safe for you and the baby) during labor and for 24 hours after delivery.
Keeping follow-up appointments after your baby is born is key. Elevated blood pressure associated with preeclampsia usually resolves on its own in the days after the baby is born, but sometimes it lingers, so you may have to take medication for a little while. If you’re at an elevated risk for preeclampsia (or if you’ve been diagnosed with it and need to monitor your blood pressure at home before or after delivery), another good option is getting a low-cost home blood pressure monitor.
Postpartum preeclampsia
It’s important to keep in mind that preeclampsia can also develop after delivery (most frequently within 48 hours of childbirth but possibly up to six weeks postpartum). The signs and symptoms, risk factors, and complications for the mother are much the same as preeclampsia developed during pregnancy, so if you notice symptoms such as severe headaches, vision changes, upper abdominal pain, or decreased urination, contact your provider right away.
Is there any way to prevent preeclampsia?
There is no clear way to prevent preeclampsia, but research has shown that women who are at high risk might benefit from taking a daily low-dose aspirin during pregnancy. This regimen is usually started late during the first trimester. If you feel that you’re at high risk for preeclampsia, talk to your provider about whether they might recommend this.
The idea of developing preeclampsia can be scary, but educating yourself about your risk factors, knowing what signs and symptoms to be on the lookout for, and getting regular prenatal care can go a long way toward identifying and treating it.
For more (technical) reading:
https://www.uptodate.com/contents/preeclampsia-beyond-the-basics
https://www.mayoclinic.org/diseases-conditions/preeclampsia/symptoms-causes/syc-20355745
https://www.mayoclinic.org/tests-procedures/labor-induction/about/pac-20385141
https://my.clevelandclinic.org/health/diseases/17733-postpartum-preeclampsia
https://www.mayoclinic.org/diseases-conditions/postpartum-preeclampsia/symptoms-causes/syc-20376646
Like this piece? Subscribe to our newsletter for real stories about women on their journey to motherhood.